Excerpted with commentary from our Range-of-Motion Testing charts. See examples of shoulder and rotator cuff pain that these tests help evaluate. See also our sampler of cervical tests from the charts and typical neck and head pain patterns coming from muscles and fascia. All these tests and more are available as a set of two wallcharts for office or dojo. Order here.
Rotator Cuff and Shoulder Girdle Tests
A "frozen shoulder" resulting from adhesive capsulitis can be less
painful and more rigid than a shoulder restricted by myofascial TrPs [trigger points].
TrPs in rotator cuff muscles, especially subscapularis,
can mimic adhesive capsulitis symptoms. On the other hand, it is not unusual for
both conditions to coexist; both need appropriate treatment.
For extensive information on differential diagnosis of shoulder and rotator cuff
problems see Travell, J. G. and Simons, D. G. (1999),Myofascial Pain and Dysfunction--
The Trigger Point Manual, Vol. 1. Available from www.Amazon.com and www.lww.com
|
Mouth
Wraparound Test
Infraspinatus |
This is the single most important
test for shoulder girdle dysfunction. Combine with Backrub
Test, below.
A. No restriction: Short upper
arms should reach corner of mouth; Normal arms: center of mouth;
Hypermobile arms: opposite side of mouth.
B. Restriction: Primarily middle deltoid/infraspinatus with
other possible involvement.If patient is:
|
|
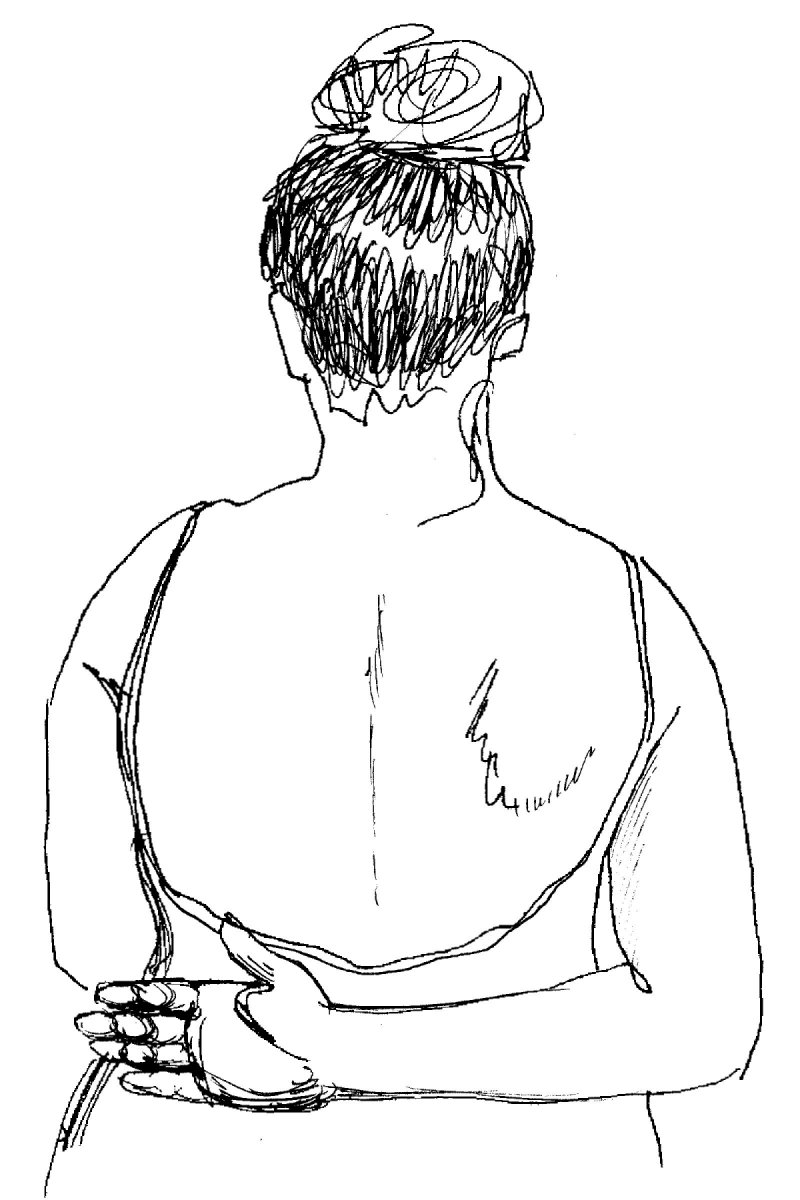
Backrub Test
Coracobrachialis |
A. No restriction: Knuckles of
palm extend beyond spine.
B. Restriction: Knuckles reach only
to midline. Restriction rare in persons of normal weight.
|
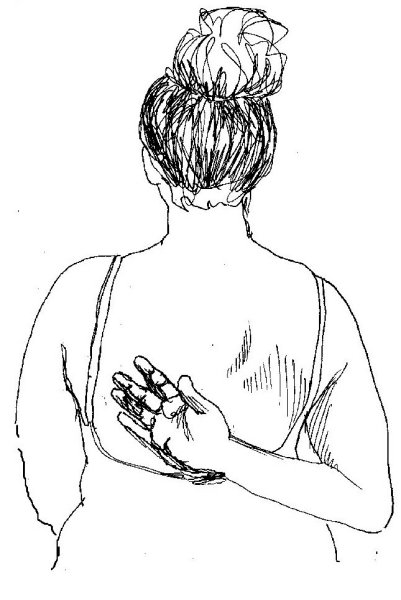
| Hand to
Shoulder Blade Test
Infraspinatus
|
Substitution: Bending wrist to reach higher up back.
A. No restriction: Fingertips reach spine of scapula.
B. Restriction: Fingertips cannot reach spine of scapula. If
patient:
|
| Overhead Reach Test
Triceps
|
Substitution: Tilting
arms away from short side to equalize
reach.
A. No restriction: Can
touch ears with insides of arms, arms reach same height, fingertips
aligned.
B. Restriction:
|
|
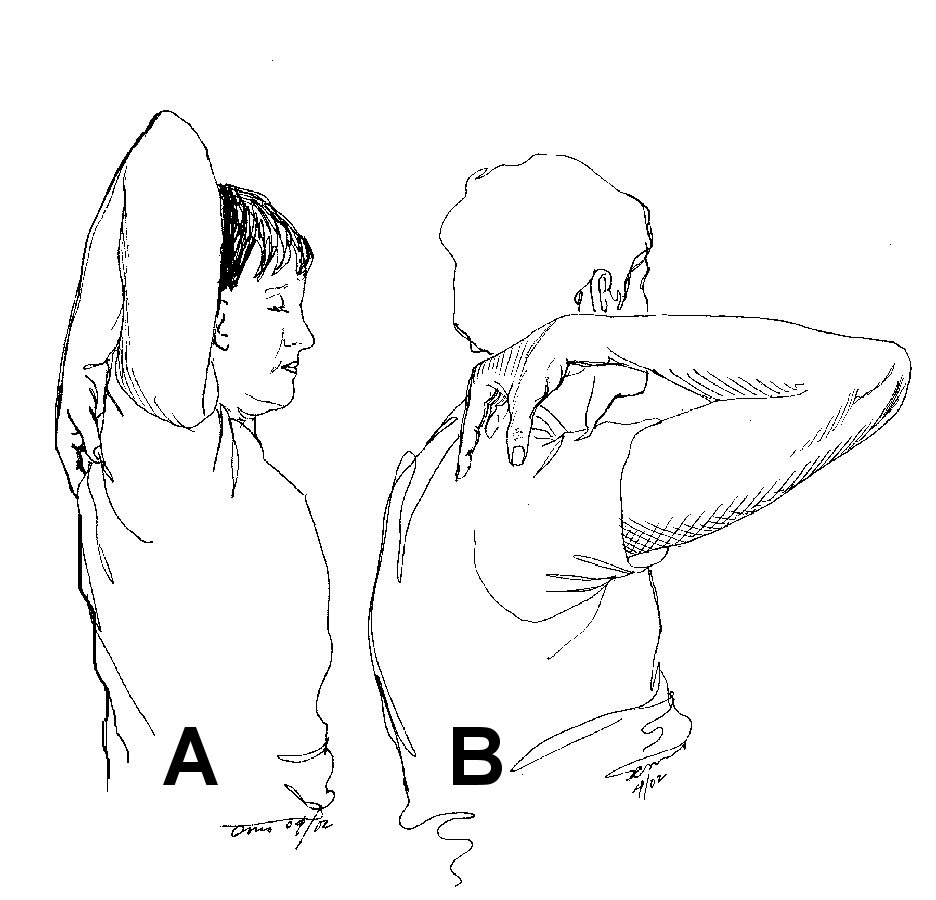
Over Shoulder Reach
Triceps
|
Substitution: Dropping head forward to bring ear forward of arm. Shifting arm out to side to relieve tightness in triceps. Keep arm and elbow perpendicular to body. A. No restriction: Elbow vertical or beyond ear. B. Restriction: Cannot point elbow to ceiling. Note: The photo from which this sketch was made was not a staged shot. It shows actual Before & After treatment range of motion. Compare active pre-treatment triceps trigger points (B) with improved range of motion immediately after treatment (A). |